



Why generic solutions fail
-
Issue with generic solutions
-
Common mistakes
What to do
-
General support strategies
-
Lifestyle recommendations
-
Nutrition recommendations
-
Supplement considerations
-
Retesting / monitoring note
The importance of gut microbiome testing
-
Why testing matters
-
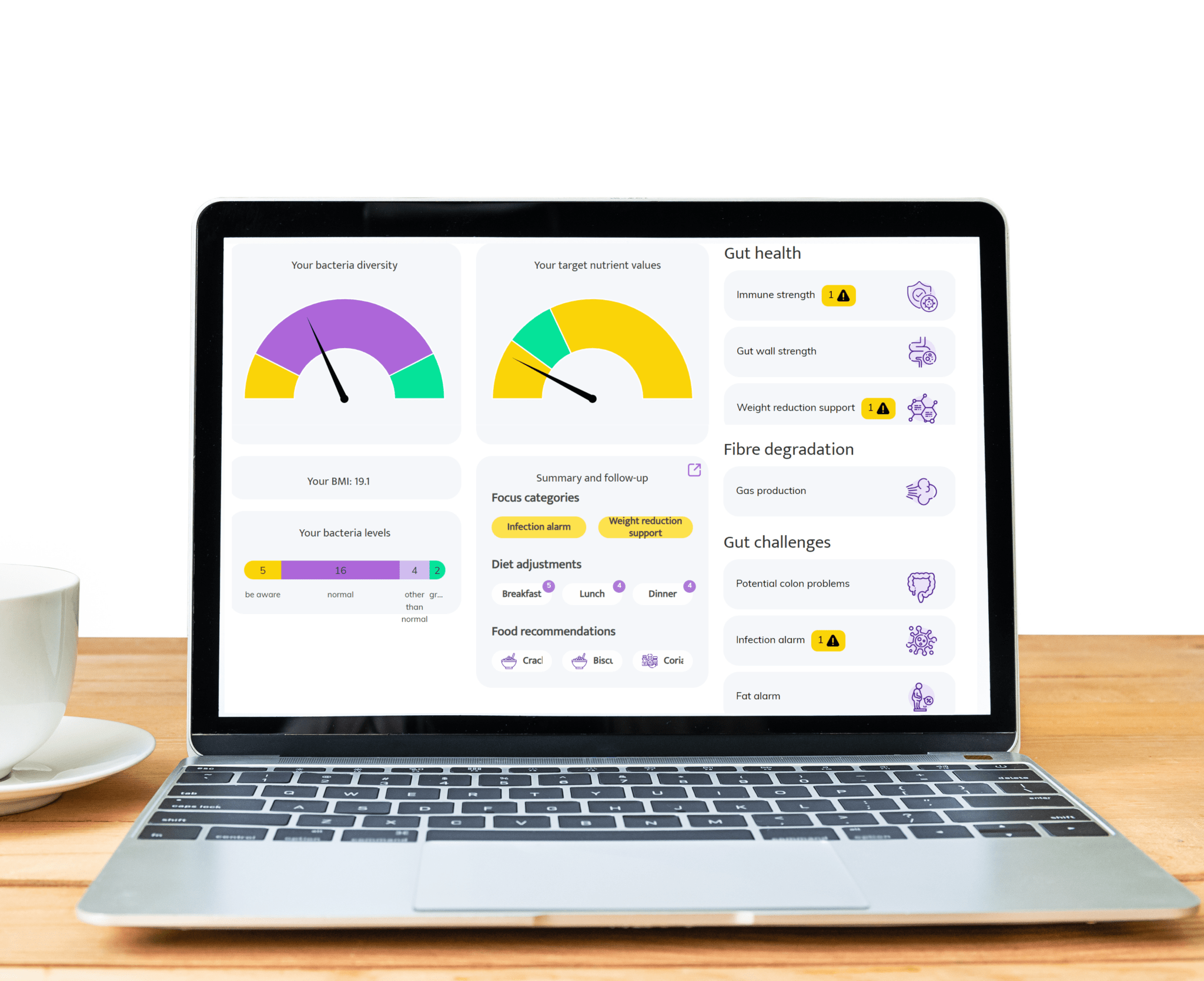
How InnerBuddies helps
Medical Evidence
-
Scientific evidence level
2 [weak—emerging evidence of association/biological plausibility; limited causal and intervention proof for clinically actionable use in cirrhosis/hepatic encephalopathy]
-
Clinical relevance note
Below is a list of the most important medical publications linked to this specific condition.
| Title | Journal | Year | Link |
|---|---|---|---|
| Alterations in the gut microbiome associated with minimal hepatic encephalopathy and cirrhosis | Hepatology | 2015 | — |
| The gut microbiota in hepatic encephalopathy is related to disease severity | Hepatology | 2014 | — |
| Rifaximin improves gut microbiome diversity and reduces endotoxemia in hepatic encephalopathy | Journal of Hepatology | 2014 | — |
| Gut microbiota dysbiosis contributes to the pathogenesis of hepatic encephalopathy | Gastroenterology | 2013 | — |
| Rifaximin reduces ammonia-producing bacteria in patients with hepatic encephalopathy | Hepatology | 2011 | — |
Frequently Asked Questions
What is hepatic encephalopathy (HE) and how is it related to the gut microbiome?
What are common signs and symptoms of HE?
How common is HE in people with cirrhosis?
What is the gut–liver–brain axis?
What does dysbiosis mean, and how does it affect HE?
What is rifaximin and how does it help with HE?
What is lactulose and how does it relate to HE management?
What is microbiome testing, and how can it help in cirrhosis/HE?
What is InnerBuddies and what does its testing provide?
Are there other microbiome-targeted therapies under study?
How can diet or lifestyle influence HE risk?
Do I need testing if I have cirrhosis or HE symptoms?
What is the difference between overt HE and minimal/covert HE?
What is the role of bile acids and ammonia in HE?
What should I discuss with my doctor about microbiome testing?
Hear from our satisfied customers!
-
"I would like to let you know how excited I am. We had been on the diet for about two months (my husband eats with us). We felt better with it, but how much better was really only noticed during the Christmas vacations when we had received a large Christmas package and didn't stick to the diet for a while. Well that did give motivation again, because what a difference in gastrointestinal symptoms but also energy in both of us!"
- Manon, age 29 -
-
"Super help!!! I was already well on my way, but now I know for sure what I should and should not eat, drink. I have been struggling with stomach and intestines for so long, hope I can get rid of it now."
- Petra, age 68 -
-
"I have read your comprehensive report and advice. Many thanks for that and very informative. Presented in this way, I can certainly move forward with it. Therefore no new questions for now. I will gladly take your suggestions to heart. And good luck with your important work."
- Dirk, age 73 -
- Choosing a selection results in a full page refresh.