



¿Por qué fallan las soluciones genéricas?
-
Problema con las soluciones genéricas
-
Errores comunes
¿Qué hacer?
-
Estrategias de apoyo general
-
Recomendaciones sobre estilo de vida
-
Recomendaciones nutricionales
-
Consideraciones sobre los suplementos
-
Nota sobre las nuevas pruebas/monitoreo
La importancia de las pruebas del microbioma intestinal
-
Por qué las pruebas son importantes
-
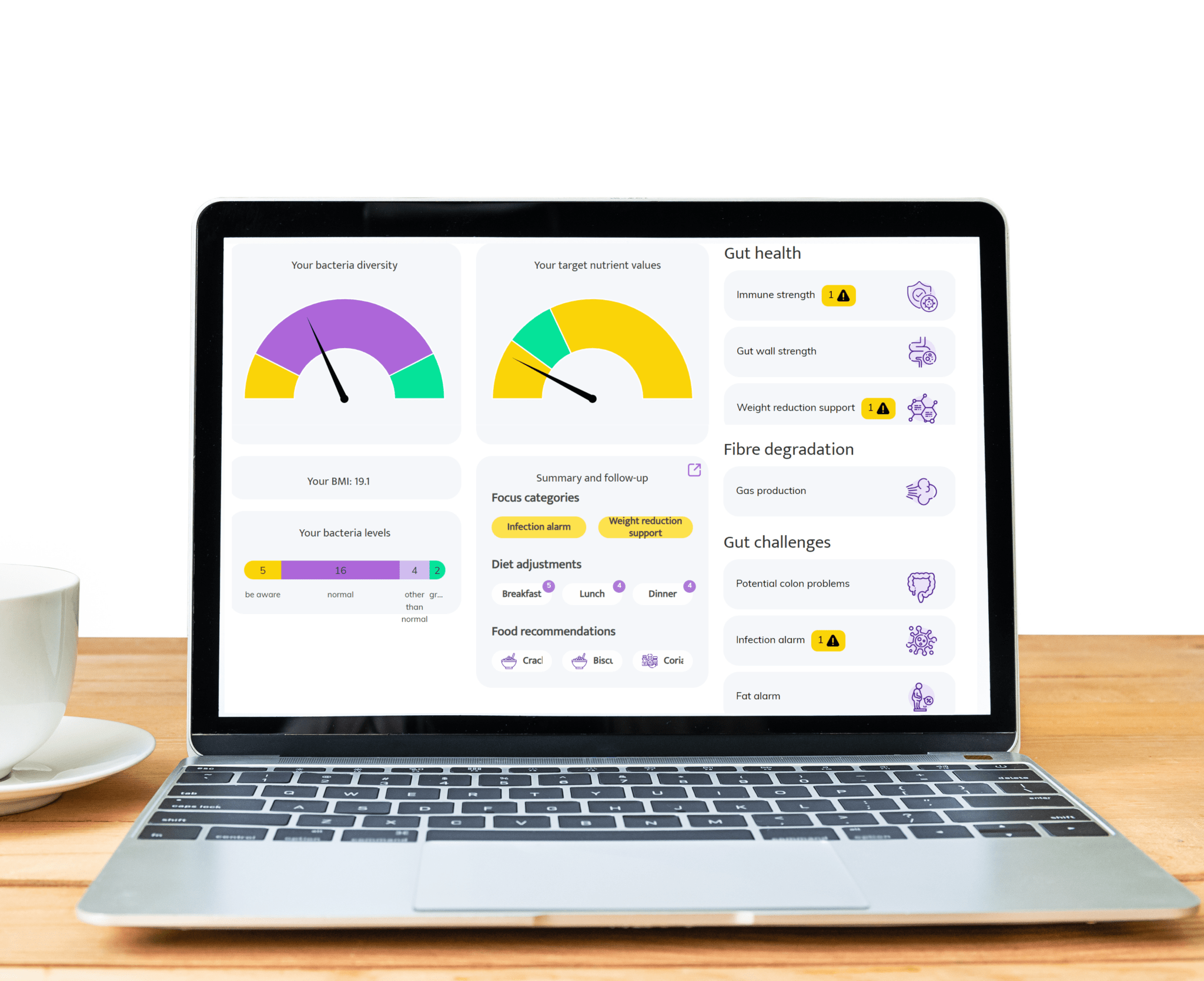
Cómo ayuda InnerBuddies
Evidencia médica
-
Nivel de evidencia científica
2 [débil; emergente pero inconsistente—principalmente asociación/plausibilidad biológica con evidencia limitada de causalidad y utilidad clínica]
-
Nota sobre la relevancia clínica
A continuación se presenta una lista de las publicaciones médicas más importantes relacionadas con esta condición específica.
| Title | Journal | Year | Link |
|---|---|---|---|
| Microbial signatures predict future colorectal cancer in a prospective cohort study | Gut | 2021 | — |
| Microbiome diversity and colorectal cancer risk: a prospective analysis | Journal of the National Cancer Institute | 2020 | — |
| Gut microbiome composition and colorectal cancer: a large-scale cohort study | Nature Medicine | 2019 | — |
| Association between gut microbiome and colorectal cancer: a meta-analysis of case-control studies | Cancer Medicine | 2019 | — |
| Gut microbiome and colorectal cancer risk: a systematic review and meta-analysis of cohort studies | Clinical Gastroenterology and Hepatology | 2019 | — |
Preguntas frecuentes
¿Qué es el microbioma intestinal y cómo se relaciona con el riesgo de cáncer colorrectal?
¿Qué microbios se asocian con mayor riesgo y cuáles son protectores?
¿Qué mecanismos conectan la disbiosis con el cáncer colorrectal?
¿Puede una prueba del microbioma predecir el riesgo de cáncer colorrectal?
¿Se recomienda la prueba del microbioma como parte del cribado?
¿Cómo influye la dieta en el microbioma y el riesgo de cáncer?
¿Qué cambios de estilo de vida pueden apoyar un microbioma más saludable?
¿Cómo complementa la información del microbioma al cribado estándar como FIT o colonoscopia?
¿Cuáles son los síntomas comunes del cáncer colorrectal y cuándo consultar?
¿Qué es el butirato y por qué es importante?
¿Existen pruebas clínicas del microbioma utilizadas hoy?
¿Cuáles son las limitaciones de la investigación actual sobre el microbioma?
¡Escucha las opiniones de nuestros clientes satisfechos!
-
"Quiero contarles lo emocionada que estoy. Llevábamos unos dos meses con la dieta (mi marido come con nosotros). Nos sentíamos mejor, pero la verdadera mejoría se notó durante las vacaciones de Navidad, cuando recibimos un gran paquete navideño y nos saltamos la dieta durante un tiempo. Eso nos motivó de nuevo, ¡porque qué diferencia en los síntomas gastrointestinales y también en la energía que teníamos los dos!" - Manon, 29 años -
-
"¡¡¡Súper ayuda!!! Ya estaba bastante bien, pero ahora sé con certeza qué debo y qué no debo comer y beber. Llevo mucho tiempo luchando contra problemas de estómago e intestinos, espero poder deshacerme de ellos ahora." - Petra, 68 años -
-
"He leído su exhaustivo informe y sus consejos. Muchas gracias, me han resultado muy informativos. Presentados de esta manera, sin duda puedo seguir adelante. Por lo tanto, por ahora no tengo nuevas preguntas. Con mucho gusto tendré en cuenta sus sugerencias. Y le deseo mucha suerte con su importante labor." - Dirk, 73 años -
- Al seleccionar una opción, se actualiza toda la página.